Frequently Asked Questions

Why 7-1-7 ?
Countries are using the 7-1-7 target and timeliness metrics to clearly assess and rapidly improve how outbreak detection, notification and early response systems are performing in real-world situations. 7-1-7 helps countries quickly and systematically surface bottlenecks to timely and effective action. Once identified, many bottlenecks can be easily addressed, and progress on those requiring longer-term efforts can be accelerated by using 7-1-7 data to prioritize action and advocate for necessary resources. Ongoing use of 7-1-7 allows countries to maintain and continue to improve their performance—the sooner threats are detected and contained; the more lives can be saved.
The 7-1-7 target was designed to be used for:
- Performance improvement: Bottlenecks are easily identified, and short and longer-term actions drive rapid, continuous improvement with every outbreak.
- Advocacy: Clear data based on simple metrics informs prioritization and shows need for resources and policy interventions.
- Accountability: Evaluating performance against simple metrics simplifies monitoring and improves transparency in reporting, making it easier to demonstrate the impact of interventions.
The 7-1-7 target is not going to address everything required for epidemic preparedness. Rather, the 7-1-7 target promotes early and effective action during outbreaks and rapid quality improvement for detection, notification, and early response systems.
The 7-1-7 target allows health officials to rapidly identify system-level bottlenecks to timely detection, notification and early response and help governments define solutions to address them. These solutions may be inexpensive and quick to implement—such as some workflow and coordination improvements—or long-term systems investments that should be prioritized in national planning efforts including National Action Plans for Health Security (NAPHS).
For example, some countries using the 7-1-7 target have identified lack of rapidly accessible funds as a bottleneck to early response. 7-1-7 performance data can be used to advocate for solutions to the lack of resources for early response, such as setting up a revolving fund for access to emergency funding, which has been shown to be effective in decreasing early response time.
In Uganda, health officials have used 7-1-7 data (in combination with data from other components of the IHR Monitoring and Evaluation Framework) to inform prioritization of activities in the national operational plan to improve epidemic preparedness. They recognized that lack of community awareness had resulted in delayed detection of certain priority diseases, such as anthrax and viral haemorrhagic fever. The 2023 Annual Operational Plan prioritized development and distribution of community educational materials for these specific diseases.
See the 7-1-7 digital toolkit for step-by-step guidance and tools
For the full scientific justification for the 7-1-7 target, please see our article published in The Lancet or read our fact sheet on the evidence base behind 7-1-7.
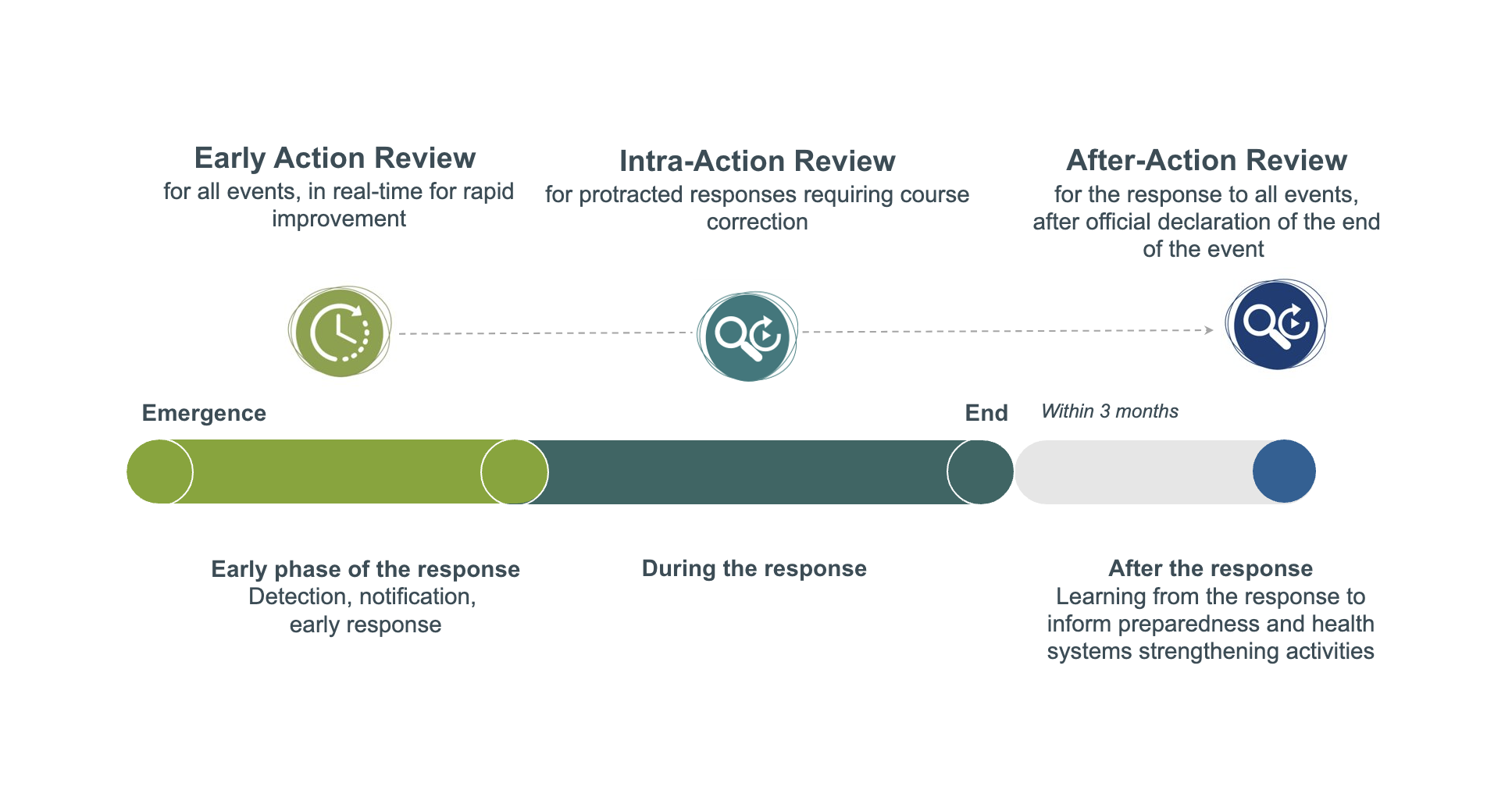
For larger events requiring a sustained response, it is best practice to apply 7-1-7 in real-time shortly after notification to identify bottlenecks and required actions for the early phase of the outbreak. At a later time, countries may conduct an Intra- or After Action Review (IAR/AAR) to identify bottlenecks and corrective actions to improve systems involved in all stages of the response. 7-1-7 results can inform these IAR and AAR discussions by highlighting the bottlenecks and corrective actions related to the early phase of the outbreak
We believe the core principles underlying 7-1-7––timeliness, real-time assessment of an event, and performance improvement––are important for and can be applied to all types of public health events. However, we recommend that the 7-1-7 target be used for infectious diseases as this target was developed for infectious diseases. 7-1-7 has at times been used for other public health events like contaminated food products; several of these investigations have started because the cause was suspected to be infectious.
The 7-1-7 target can be applied to any infectious disease outbreak event. While there are differences between diseases, the aim in selecting a single target across diseases was to simplify and standardize assessment of the systems involved in outbreak event detection, notification, and early response. This helps 7-1-7 keep the focus on its primary goal of improving system-level performance by using simple and clear timeliness metrics to identify bottlenecks that delay appropriate action and completing corrective actions to resolve them.
While rapid detection and response actions are more easily accomplished for some pathogens than others, a review of timeliness across various diseases, and the subsequent piloting of 7-1-7 in various countries across many disease types, have supported the notion that the 7-1-7 target is ambitious but achievable for most infectious diseases. For the small number of diseases where, say, detection within 7 days may be rarely or not possible, the focus would still be on finding areas to improve speed as 7-1-7 is first and foremost about performance improvement.
Stratifying data by disease type is a simple way to add nuance and epidemiological context, if needed, when discussing timeliness results by disease type.
How 7-1-7 fits in
Timeliness has been increasingly recognized as an important factor in improving system performance for early detection and response to public health emergencies.
The 7-1-7 target was incorporated to the WHO’s Fourteenth General Programme of Work for 2025-2028 as a joint outcome indicator. 7-1-7 is also aligned with Triple Billion target for Health Emergencies Protection, which created a new global metric for the timely detection, notification and response to public health threats.
It also contributes to the achievement of Sustainable Development Goal 3, specifically target 3.3, which aims to end epidemics of communicable diseases and strengthen country capacity for early warning, risk reduction and management of national and global health risks.
The Pandemic Fund, which provides grant financing for projects that seek to strengthen pandemic prevention, preparedness and response functions, also included the 7-1-7 target in its results framework.
The 7-1-7 target offers a complementary approach and proposes a simplified way of assessing how well health security systems detect and respond to disease outbreaks in real-world conditions and real time. It helps countries gather reliable data for immediate decision-making to improve overall coordination and performance and prioritize their use of existing resources and future funding needs.
The revised International Health Regulations (2005) (IHR) were established to ensure global security and help countries build the capacities needed to detect and respond to public health emergencies. As the global experience with COVID-19 made clear, too many countries were not adequately prepared for a pandemic, even when they seemed prepared on paper.
Capacity assessments are crucial for preparedness and health security, but can also be abstract, time-consuming and resource intensive. Reviewing real-world performance using the 7-1-7 target can be done routinely and delivers immediately actionable data. It’s a quick but comprehensive evaluation of how well detection, notification, and response systems are working during the early phase of an outbreak, using a systems approach focused on identifying bottlenecks and enablers to timely performance. Detection, notification, and response systems can then be improved, both rapidly and over the longer-term, using real-world data on performance to prioritize activities and resources where they’re needed most.
In many settings, effective implementation of National Action Plans for Health Security (NAPHS) and annual operational plans designed to improve countries’ core capacities has been handicapped by a lack of prioritization. Integrating 7-1-7 recommendations into these plans’ development process identifies focal areas for performance improvement and helps define a more feasible number and order of priorities per IHR technical area for both implementation and funding. When done alongside other tools and assessments, this helps create more robust recommendations for prioritization.
The 7-1-7 target also complements existing preparedness assessments under the IHR, including the State Parties Self-Assessment Annual Reporting (SPAR) and Joint External Evaluation (JEE) tools, by evaluating the efficacy of outbreak detection, notification, and early response systems under the pressure of real-world conditions.
The 7-1-7 target is the bedrock of guidance from the World Health Organization (WHO) on Early Action Reviews (EARs), providing clear performance targets and a simple way to check performance from the very start of a public health event rather than months later. WHO encourages countries to incorporate EARs into their existing response frameworks and through their existing response coordination structures. 7-1-7 data from an EAR can then be incorporated into and enhance Intra-Action reviews (IARs) and After-Action Reviews (AARs) for prolonged and/or large outbreaks.
 The 7-1-7 target and its associated performance improvement methodology and tools are the bedrock of EARs. An EAR uses 7-1-7 to assess infectious disease outbreak events in real time, and identify bottlenecks and corrective actions that can result in system-level improvements. The WHO’s EAR guidance provides stepwise instructions to support the implementation of EARs.
The 7-1-7 target and its associated performance improvement methodology and tools are the bedrock of EARs. An EAR uses 7-1-7 to assess infectious disease outbreak events in real time, and identify bottlenecks and corrective actions that can result in system-level improvements. The WHO’s EAR guidance provides stepwise instructions to support the implementation of EARs.
For prolonged or larger outbreaks that result in IARs or AARs, EARs can be used to help inform these reviews by focusing on the timeliness, bottlenecks, and corrective actions that can improve systems relevant to the early phase of the outbreak.
An Early Action Review (EAR), which leverages the 7-1-7 target, has similarities with an AAR to the extent that both focus on performance improvement by trying to understand what worked and didn’t work during an outbreak and what can be improved going forward. EARs and 7-1-7 focus on detection, notification, and response actions undertaken within the early phase of an outbreak. They can be used for immediate and real-time evaluation of both small and large events, while AARs are typically only conducted for large events and after the event is over.
7-1-7 and AARs are complementary and may both be performed on the same event. 7-1-7 findings can be used to inform AAR discussions on the early phase of the event. WHO’s country implementation guidance for AARs includes the timeliness metrics on which the 7-1-7 target was based. Most importantly, recommendations from both types of performance reviews should be included in national planning to prioritize and accelerate implementation of corrective actions.
Using 7-1-7 yields improved documentation of the events leading up to a larger outbreak. It helps surface early barriers to detection, notification, and response in events that resulted in a larger-scale emergency requiring an AAR. The performance metrics for 7-1-7 allow for specific types of bottlenecks and actions to be prioritized for discussion during the AAR and subsequent integration into follow-up planning.
Prior to the AAR, a 7-1-7 analysis of the event should be conducted. Ideally, this would have been done through an Early Action Review (EAR) in real-time during the early phase of the outbreak. Otherwise, it can be done retrospectively. See detailed guidance on how 7-1-7 findings can then be used to inform discussions during an AAR, including how 7-1-7 findings align with different steps of AARs. See also the 7-1-7 event review template, which can be used to consolidate 7-1-7 findings for an event.
Overall, the 7-1-7 target supports IDSR implementation by:
- Simplifying measurement of performance
- Evaluating the performance of IDSR systems involved in event detection, notification and early response
- Identifying performance gaps and bottlenecks that require corrective action to strengthen IDSR implementation.
The WHO AFRO IDSR 3rd Edition Technical Guidelines (2019) include sample indicators for timely detection, notification, and response. These have been translated at country level but not fully implemented for monitoring and evaluation. The 7-1-7 target was designed to align with and simplify measurement of timeliness in the IDSR:
- The 7-days-to-detect metric aligns with the IDSR: “Cumulative interval between onset of index case (or occurrence of an unusual cluster at the community or health facility [date 1] and notification to the district [date 2] (target <7 days))” [IDSR Section 7, p. 142]
- The 1-day-to-notify metric aligns with the IDSR: “If an immediately reportable disease, condition, or other public health event is suspected, the health facility must report case-based information to the next level within 24 hours” [IDSR Section 2, p. 57]
- The 7-days-to-complete-an-early-response metric is an extension of the IDSR, which calls for action to be taken within 48 hours of notification. The 7-1-7 target includes a response measurement: completing all seven early response actions. These 7 early response actions constitute the core response actions typically needed in response to both smaller and larger public health events. As described in our fact sheet on the evidence base behind 7-1-7, seven days for early response action completion was considered to be an ambitious but achievable target for most events. Although not a part of core 7-1-7 data collection, countries can also collect data on how soon after notification the response was initiated if they wish.
The 7-1-7 target uses simple metrics to measure performance in countries implementing IDSR, which in turn improves accountability and transparency. For these reasons, WHO AFRO adopted the 7-1-7 target in its Regional Strategy for Health Security and Health Emergencies 2022-2030.
Ideally the 7-1-7 target is adopted and used across relevant One Health sectors, and regular stakeholder engagement is facilitated through multisectoral, One Health government mechanisms. This systems integration allows One Health partners to consistently evaluate the 7-1-7 target for zoonotic diseases, including identifying which sector first detected the disease and when multisectoral notification was initiated.
In addition, sectors can collaborate on joint early response actions, including when to deploy multisectoral rapid response teams, how to conduct joint risk assessments, initiate lab confirmation, infection prevention control, and consistent risk communication.
The 7-1-7 Alliance
The 7-1-7 Alliance is a country-led partnership that accelerates and supports achievement of the 7-1-7 target.
Founded in February 2023, the Alliance is open to national, regional and local governments, public health and research institutions, multilateral agencies, civil society organizations, and donors and foundations.
Our main activities include:
- Providing ongoing technical assistance for performance improvement through 7-1-7 and the World Health Organization’s Early Action Reviews, which leverage 7-1-7
- Engaging partners in communities of practice and regional learning networks to strengthen implementation, disseminate lessons learned and further refine the 7-1-7 approach
- Developing resources and maintaining an online hub with guidance, tools and training materials to support implementation
- Advancing operational research and learning
- Establishing a common monitoring and evaluation agenda to improve in-country planning and implementation processes and inform donor funding priorities.
The secretariat for the 7-1-7 Alliance is hosted by Resolve to Save Lives for an initial five-year period.
The Alliance also benefits from the strategic advice of a Technical Steering Group composed of country representatives, multilateral partners and technical experts.
The 7-1-7 target was initially piloted in Brazil, four jurisdictions in the U.S, and four African countries (Ethiopia, Liberia, Nigeria, Uganda) with support from Resolve to Save Lives and the Bill & Melinda Gates Foundation. Findings from the pilots have shown that the 7-1-7 target is feasible across high, middle and low-income countries and can improve health security system performance. Using 7-1-7 helps identify problems and bottlenecks that have been missed in other evaluations, many of which can be rectified in real time for little or no cost.
7-1-7 is now in use in a growing number of other countries across Africa, Asia and South America.
The 7-1-7 Alliance hosts a global community of practice where country experts learn from their peers and discuss best practices, successes and challenges.
If your country is ready to adopt or is already using the 7-1-7 target and/or Early Action Reviews, please fill out an application to join the community of practice.
The 7-1-7 Alliance is working with countries and technical partners to leverage large external funding mechanisms, such as the Pandemic Fund, World Bank Multi-phase Awards, Global Fund COVID-19 Response Mechanism, and more. Many of these funding mechanisms have integrated the 7-1-7 target into their impact and results frameworks and provide an important opportunity to leverage large-scale funding to support sustained use of 7-1-7.
The 7-1-7 Alliance is able to support countries that have applied for or received funding from such mechanisms to adopt and implement 7-1-7. Support includes ongoing technical assistance, engagement with other implementing partners through our Community of Practice and Global Learning Network, suite of adoption and implementation tools as well as our data and monitoring and evaluation framework.
Countries that are applying for those funding opportunities are encouraged to read this technical brief with actionable guidance on adding 7-1-7 to their proposals and the cost estimates associated with 7-1-7 adoption, and to watch this webinar on how to build 7-1-7 into Pandemic Fund proposals.
Adopting and using 7-1-7
For most countries or jurisdictions, initial steps will include:
-
- Situating 7-1-7 within the public health system (e.g. identifying which team will lead 7-1-7 coordination)
- Mapping out relevant stakeholders in the country/jurisdiction and existing systems used in workflows relevant to 7-1-7
- Introducing the 7-1-7 target to a broad set of stakeholders, including high-level decision-makers and those working in the areas of coordination, data collection, performance improvement, national planning, and communications and advocacy
- Integrating 7-1-7 into existing workflows, including for data collection, stakeholder meetings, and national planning
- Training staff
- Piloting the use of 7-1-7 and iterating as needed.
Several countries have also employed a dedicated staff-person to support the first year of implementation, with responsibilities including supporting the above adoption steps, developing an implementation plan, updating guidance, convening stakeholders, and consolidating 7-1-7 performance data. Once these initial steps have been completed, the workload decreases, and ongoing 7-1-7 implementation may not require full-time dedicated staff.
See guidance and tools for adopting 7-1-7 into a country or jurisdiction’s routine systems. After adoption, the country should be ready to regularly use 7-1-7 for outbreak events, including in real-time for Early Action Reviews. See guidance and tools for using 7-1-7.
There is no single answer for how and where the 7-1-7 target is adopted in a country. This decision depends on several factors, including the governance structure in the country and political will.
One option that several countries have used is to first implement 7-1-7 at the national level, with the team leading implementation sitting at that level (e.g., at the national public health emergency operation center) and coordinating 7-1-7 activities from this level. Then, once implementation is robust at the national level, 7-1-7 adoption and use can be scaled to the subnational level. This allows for a strong national foundation that can support effective implementation at other levels in the country. Countries across the spectrum of centralized to decentralized federal systems have used this model for 7-1-7 adoption and use.
Another model that has been used, especially in countries with decentralized governance systems like Brazil and the United States, has been to adopt and use 7-1-7 in select jurisdictions, with momentum building towards national support. This has allowed jurisdictions to start using 7-1-7 when they are ready, while demonstrating its potential within the country, building political will, and identifying ways in which the national level can support 7-1-7 adoption and use.
Whether adoption begins at the national level or subnational level, ideally the different levels of government that are involved in outbreak detection, notification, and response––from the national to the local––will be engaged in 7-1-7 over time.
A country should first go through the steps for adopting 7-1-7 into its routine systems. See guidance and tools for this. After adoption, the country should be ready to regularly use 7-1-7 for outbreak events, including in real-time for Early Action Reviews. See guidance and tools for using 7-1-7.
Each country must decide on the roles that different levels of the public health system will have in using the 7-1-7 target. When determining roles and responsibilities, considerations should include which levels of the public health system are expected to be immediately notified of a new public health event, which levels of government are typically responsible for the seven early response actions including the initial investigation, which levels of government possess the financial resources to resolve bottlenecks during an ongoing response, and which levels of government are involved in developing National Action Plans for Health Security or other operational plans that identify what is needed to improve the systems involved in detection, notification, and response.
In most settings where the 7-1-7 target is being used, responsibility for the initial investigation and response lies at the local level (e.g., municipal, district). It has therefore been deemed important to train relevant staff, for example rapid response teams, at this level to use the approach. Higher levels of government have typically provided technical and financial support to the local level. Convening higher level stakeholders shortly after notification, to review progress towards completing the seven early response actions, can be instrumental in accessing the resources needed to address bottlenecks and improve the ongoing response. In addition, higher levels of government can use the 7-1-7 target to monitor the performance of local public health jurisdictions and identify those requiring additional support, as well as identifying bottlenecks common to multiple jurisdictions that require prioritized action.
Civil society organizations (CSOs) and communities play a critical role in helping countries and jurisdictions achieve the 7-1-7 target through advocacy, accountability, and community engagement. CSOs can help hold health systems accountable, from local health facilities to national governments, while advocating for stronger, more responsive public health systems.
CSOs can also complement government efforts by reaching underserved populations, promoting awareness of the importance of early reporting, and supporting best practices for outbreak detection and containment.
Community health actors also contribute to early detection through local surveillance and trusted community networks. Together, these efforts help build a community-centered public health ecosystem that supports timely detection, reporting, and response to health threats.
This is especially relevant as countries that have adopted 7-1-7 at the national level roll out 7-1-7 subnationally. Countries that have applied 7-1-7 separately in different jurisdictions for the same outbreak as it has spread have found important differences in timeliness and bottlenecks across the jurisdictions, thus adding nuance to which corrective actions are needed and where they are needed.
Detection
The date the clinician identified a suspected case that meets the definition for reporting would be the date of detection. It does not matter if the true etiology ends up being different from that initially suspected. This includes any type of disease cluster that meets guidelines for reporting, including those of unknown etiology.
In all settings, we recommend using the first threshold that, once exceeded, should trigger a public health investigation or response according to existing guidelines and standard operating procedures (SOPs). Generally, we anticipate that the “alert” thresholds will be used, given that the IDSR Technical Guidelines Third Edition states that “an alert threshold suggests to health staff and the surveillance team that further investigation is needed.” The alert threshold may be based on suspected and/or confirmed case incidence depending on reporting guidelines.
Notification
The date of notification is the date the information reaches the first public health authority who is responsible for action. This will depend on how governance in the country/jurisdiction is set up. In many cases, this is at the local/district level. In some cases, it may go straight to the national level.
For jurisdictions whose guidelines require immediate simultaneous notification to multiple levels of government, reviewing if notification to all levels meets the 1-day target may be useful for identifying additional bottlenecks and corrective actions. However, when calculating 7-1-7 performance, the earliest date on which a level of government responsible for action was notified should be used.
Notification refers to any event that a country or other jurisdiction determines to be notifiable. Existing guidelines should describe what events are notifiable based on, for example, suspected cases, confirmed cases, or events beyond human health such as clusters of animal deaths. Clear guidance defining notifiable events are critical for 7-1-7 implementation. The 7-1-7 target can also be used to identify when guidelines are not sufficiently specific and would benefit from improved reporting definitions; this can be discussed in the stakeholder meetings when findings from 7-1-7 are presented.
Early response
Several of the 7-1-7 early response actions are defined by initiation of the activity (e.g. “Initiate appropriate public health countermeasures in affected communities”). For those, the milestone date is based on when the activity was initiated. The ‘date of early response action completion’ is the last milestone date across the seven early response actions.
The 7-1-7 early response actions are:
- Initiate investigation or deploy investigation/response team
- Conduct epidemiologic analysis of burden, severity and risk factors, and perform initial risk assessment
- Obtain laboratory confirmation of the outbreak etiology
- Initiate appropriate case management and infection prevention and control (IPC) measures in health facilities
- Initiate appropriate public health countermeasures in affected communities
- Initiate appropriate risk communication and community engagement activities
- Establish a coordination mechanism
Whenever possible, estimates of when actions occurred should be based on available data. If no estimates are available, the early response should be considered completed on the last known date when an early response action was completed. However, in documents and presentations of the event, it will be important to document that a date could not be determined, in order to promote discussion on how data collection can be improved.
In 7-1-7, the 7-day response target is defined as the time to complete specific early response actions, including risk communication and community engagement. In the 7-1-7 Milestone Dates Reference Guide, outbreak declaration is included as one of the actions that can be used to document the date that risk communication and community engagement actions were initiated. Notably, some outbreaks may not have a formal declaration, such as smaller clusters or endemic diseases crossing the predetermined thresholds.
The key determinant is deciding if the action done on day 30 should have been undertaken as part of the early response. At times, an early response action may not be appropriate for the initial response, but may become appropriate at a later time after the event has changed or the outbreak has spread. It is up to stakeholders to determine, based on their professional judgment, if an action should have been done as part of the early response or if that action was not initially applicable. If the action completed on day 30 should have been done as part of the early response, then recording 30 days for the early response action completion milestone would be appropriate. If the action completed on day 30 would not have been appropriate as part of the early response, but became necessary later, then recording the latest date of the other relevant early response actions (e.g., 5 in this case) would be appropriate.